Health Care
Kaitlyn Finley | February 20, 2020
Price transparency—not welfare expansion—the key to health care reform
Kaitlyn Finley
Decades of rising health care prices have turned financial headaches into looming financial insolvency for many American families. Despite massive efforts to fix health care by pumping more federal subsidies into health insurance under Obamacare, nearly half of Americans believe a major medical expense could leave them bankrupt, according to a recent Gallup poll.
In Oklahoma, efforts are under way to further expand federal control over Oklahoma’s health care system through Medicaid expansion. Under Obamacare, states may expand their Medicaid programs to certain low-income able-bodied adults, receiving additional federal reimbursement funding (with states paying 10 percent of costs).
Proponents of Medicaid’s expansion to hundreds of thousands of able-bodied adults claim it will lower costs for all Oklahomans. They argue that adopting Medicaid expansion will save rural health care in Oklahoma and lower insurance costs, since nonprofit hospitals will no longer have to shift uncompensated charity care to private payers.
These claims have not held water. Obamacare Medicaid expansion in other states has cost taxpayers 157 percent more than what was projected by state officials, according to the Foundation for Government Accountability.
Recent academic studies of California, Colorado, and Arizona have shown Medicaid expansion failed to reduce urban hospital service prices (with Colorado’s hospitals raising prices and profit margins) or insurance premiums, nor did it have a significant positive effect on health outcomes.
Based on data commissioned by the Oklahoma Health Care Authority, as well as the experiences of other expansion states, if Oklahoma expanded Medicaid to all 628,000 potential able-bodied enrollees, Oklahoma taxpayers could be on the hook for nearly $375 million annually.
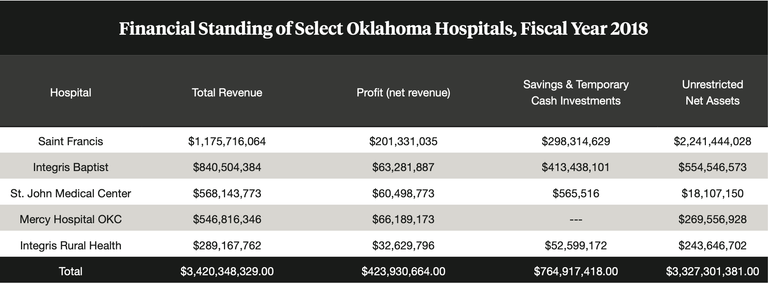
Source: ProPublica Nonprofit Explorer, Forms 990 data, methodology based on Dr. Byron Schlomach and Baylee Butler's work, The Profitability of Nonprofit Hospitals: Do They Really Need More Money? 1889 Institute, September 2017
It’s clear that expanding Medicaid and other attempts to increase “coverage” will not accomplish what Americans need most—lowering health care bills.
As Dr. Martin Makary, a professor of surgery at the Johns Hopkins University School of Medicine and author of the book The Price We Pay: What Broke American Health Care—and How to Fix It, recently summarized: “We don’t have an insurance crisis in the United States. We have a pricing crisis. We have a cost crisis. What we are hearing about from Washington is really different ways to finance the broken health care system, not how to fix the broken health care system.”
State lawmakers should address the lack of price transparency for patients. Due in part to the lack of price transparency, hospital service prices continue to outpace inflation. Patients must worry they will be hit with a surprise out-of-network charge, despite having insurance. Twenty percent of emergency room visits in Oklahoma resulted in at least one out-of-network charge in 2017 (two percent higher than the national average), according to a recent study by the Peterson Center on Healthcare and the Kaiser Family Foundation.
Many hospitals in Oklahoma recently ramped up efforts to fully collect their trumped-up charges from patients. Last August, Oklahoma Watch reported that 22,250 lawsuits were filed against former patients by Oklahoma hospitals from 2016 to July 2019, more than half filed by large hospitals in Oklahoma City and Tulsa. If patients fail to pay or dispute charges, they may have their wages garnished, hurting their credit score.
As shown in the nearby table, according to their latest federal filings, Oklahoma’s five largest hospitals generated $3.4 billion in revenue and pocketed $423 million in profit. They hold $764 million in cash and temporary cash investments, with unrestricted net assets totaling $3.3 billion.
To promote price transparency and mitigate lawsuits pursued by large hospital corporations, lawmakers should support Senate Bill 1646, which would prevent hospital providers from reporting medical debt to credit collectors when patients had not first reviewed and agreed to charges before services were rendered.
In contrast to large hospital systems in Oklahoma’s metroplexes, rural health care may need additional funding. It’s true that a sliver of Medicaid expansion funds would go to rural areas, but most dollars would stay in rich metro hospitals. Instead of giving metro hospitals a blank check signed by Oklahoma taxpayers, lawmakers should direct available funds to rural health care infrastructure.
House Joint Resolution 1017 would direct future tobacco-settlement payments to help struggling rural hospitals. A portion of this money could be used to pay for medical school students who agree to practice in rural areas upon graduation, ensuring Oklahoma increases the number of providers in areas with the most need.
The evidence shows that more welfare expansion, more government intrusion, and more taxpayer dollars in health care just cause more dollars to chase the same services. Oklahoma policymakers should promote legislation that unshackles the free market—promoting price transparency and competition to reduce health care costs—rather than expand the number of taxpayer dollars swallowed by health care.

Kaitlyn Finley
Policy Research Fellow
Kaitlyn Finley currently serves as a policy research fellow for OCPA with a focus on healthcare and welfare policy. Kaitlyn graduated from the University of Science and Arts of Oklahoma in 2018 with a Bachelor of Arts in Political Science. Previously, she served as a summer intern at OCPA and spent time in Washington D.C. interning for the Heritage Foundation and the U.S. Senate Committee on Environment and Public Works.