Culture & the Family
Ray Carter | March 26, 2020
States’ COVID-19 responses based on faulty data?
Ray Carter
In Oklahoma and nationwide, government officials have often pointed to graphs showing the predicted impact of COVID-19/coronavirus, highlighting dramatically different outcomes based on whether dramatic state-ordered restrictions are imposed on the populace.
Yet one source for many of those charts—the organization COVID Act Now—is now coming under fire for questionable methodology that critics say makes many dire predictions dubious.
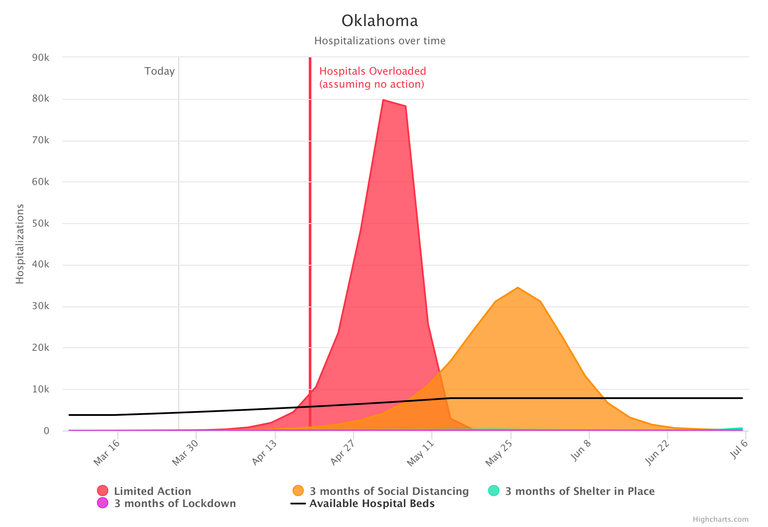
The website for COVID Act Now’s Oklahoma projections includes both alarming forecasts—and major caveats.
As of March 25, state officials report that 59 Oklahomans have been hospitalized for COVID-19. COVID Act Now predicts that figure will rise to 79,717 by May 2 under a scenario in which “no action” is taken, declaring that the point when hospitals will be “overloaded.”
However, social distancing and other measures have been in place for the past two weeks. Under COVID Act Now’s “social distancing” model, the organization predicts the number of Oklahomans hospitalized as a result of the virus will hit 34,483 by May 26 and then decline.
The site declares, “To prevent hospital overload, Shelter in Place must be implemented” by April 5 to April 10 in Oklahoma and predicts such an order would result in just 1 percent of the Oklahoma population becoming infected and less than 1,000 deaths. With social distancing, the site claims around 70 percent of Oklahomans will be infected and 58,000 will die.
Yet the site includes major caveats that suggest those predictions are as much fiction as fact. At the top of the website, COVID Act Now declares, “This model is intended to help make fast decisions, not predict the future.”
On the webpage discussing its model, COVID Act Now concedes that since this is a new disease, variables “will change.” The organization also describes its predictions for the impact of interventions as “guesses, in some cases informed by data.”
The organization’s model “does not adjust for the population density, culturally-determined interaction frequency, and closeness, humidity, temperature, etc.”
COVID Act Now’s analysis also “assumes everyone spreads the disease at the same rate,” which the organization concedes is not accurate.
Furthermore, COVID Act Now says its data regarding demographics, populations, and hospital bed counts “are outdated.”
“Demographics for the USA as a whole are used, rather than specific to each state,” the site declares.
The flaws of COVID Act Now’s model have become increasingly apparent in recent days. The Federalist recently reported that COVID Act Now’s “predictions have already been proven to be wildly wrong.”
The Federalist noted that COVID Act Now predicted Tennessee would have 190 hospitalizations by March 19. Instead, that state experienced just 15 by that date.
In New York, COVID Act Now predicted nearly 5,400 New Yorkers would be hospitalized by March 19. The real number was around 750. By March 23, COVID Act Now predicted nearly 13,000 New York citizens would be hospitalized. The actual number was around 2,500.
In Georgia, The Federalist reported that COVID Act Now predicted 688 hospitalizations by March 23, but fewer than 300 were hospitalized by that date.
In Florida, COVID Act Now predicted 400 hospitalizations by March 19. Instead, around 90 were hospitalized by that date.
“COVID Act Now’s models in other states, including Oklahoma and Virginia, were also far off in their predictions,” The Federalist reported.
The Texan reports that the Texas Chapter of the Association of American Physicians & Surgeons has also criticized the COVID Act Now model, saying it “has a number of limitations and is likely to be an exaggerated estimate of deaths for the state of Texas. It does not take into account the limitations of the available data, which include selection bias due to limited number of tests, high false positives and false negatives of the test widely used, differences in social structure, population density, population health and risk factors such as smoking among the nations reporting data.”
The Texan also reports that COVID Act Now’s medical advisor, Nirav Shah, is an adjunct professor of medicine in primary care and population health at Stanford University but “is not an epidemiologist or specialist in public health responses.”
For this article, the offices of the governor, the mayor of Oklahoma City and the mayor of Tulsa were all contacted by email and asked if COVID Act Now’s materials were utilized in the decision-making processes of those offices. As of publication, none had responded.

Ray Carter
Director, Center for Independent Journalism
Ray Carter is the director of OCPA’s Center for Independent Journalism. He has two decades of experience in journalism and communications. He previously served as senior Capitol reporter for The Journal Record, media director for the Oklahoma House of Representatives, and chief editorial writer at The Oklahoman. As a reporter for The Journal Record, Carter received 12 Carl Rogan Awards in four years—including awards for investigative reporting, general news reporting, feature writing, spot news reporting, business reporting, and sports reporting. While at The Oklahoman, he was the recipient of several awards, including first place in the editorial writing category of the Associated Press/Oklahoma News Executives Carl Rogan Memorial News Excellence Competition for an editorial on the history of racism in the Oklahoma legislature.